

If you’ve experienced a panic attack, you already know it doesn’t feel like “just anxiety.” Your heart hammers. Your chest tightens. Your brain fires off worst-case scenarios at full volume. And somewhere in the middle of all of it, a terrifying thought surfaces: What if this never gets better?
It can get better. But here’s what most generic therapy guides won’t tell you: not every therapy works the same way for panic. Choosing the wrong approach — or defaulting to supportive talk therapy that never directly touches the panic cycle — is one of the main reasons people spend years in treatment without real relief.
At the Calm Anxiety CBT Therapy Clinic in Chicago’s Lakeview neighborhood, we treat anxiety and panic disorder every day — with clients coming in from Lincoln Park, the Loop, River North, and across Illinois via telehealth. What we’ve found consistently is that the most effective treatment isn’t about finding the “best” therapy in the abstract. It’s about understanding exactly how panic works — and matching the right tool to the right stage of the cycle.
That’s what this guide is built around. We’ll walk through the CBT panic cycle — the five-stage loop that keeps anxiety and panic locked in place — and map each major evidence-based therapy to the specific stage it targets most powerfully. By the end, you’ll have a much clearer picture of what therapy is actually addressing your experience, and what to look for when choosing a Chicago anxiety therapist who specializes in panic.
If you’re still working out whether what you’re experiencing is anxiety, panic, stress, or something else, our post on the difference between stress, anxiety, and depression is a useful starting point before diving in here.
? The CBT Panic Cycle: Why Panic Keeps Coming Back
Panic disorder isn’t random. It follows a predictable loop — one that Cognitive Behavioral Therapy has spent decades mapping and targeting with precision. Understanding this cycle is the first step toward breaking it, and it’s the framework we use at the Calm Anxiety Clinic to organize every panic treatment plan we build.
The five stages of the CBT panic cycle:
- Trigger — A situation, sensation, or thought activates your threat system
- Physical Sensation — Your body responds: racing heart, shortness of breath, dizziness, chest tightness
- Catastrophic Thought — Your brain interprets those sensations as dangerous: “I’m having a heart attack.” “I’m going to lose control.” “I’m going to pass out in front of everyone.”
- Fear of Fear — You become afraid of the panic itself, scanning constantly for early warning signs that it’s coming
- Avoidance — You begin structuring your life around preventing panic: avoiding places, sensations, situations
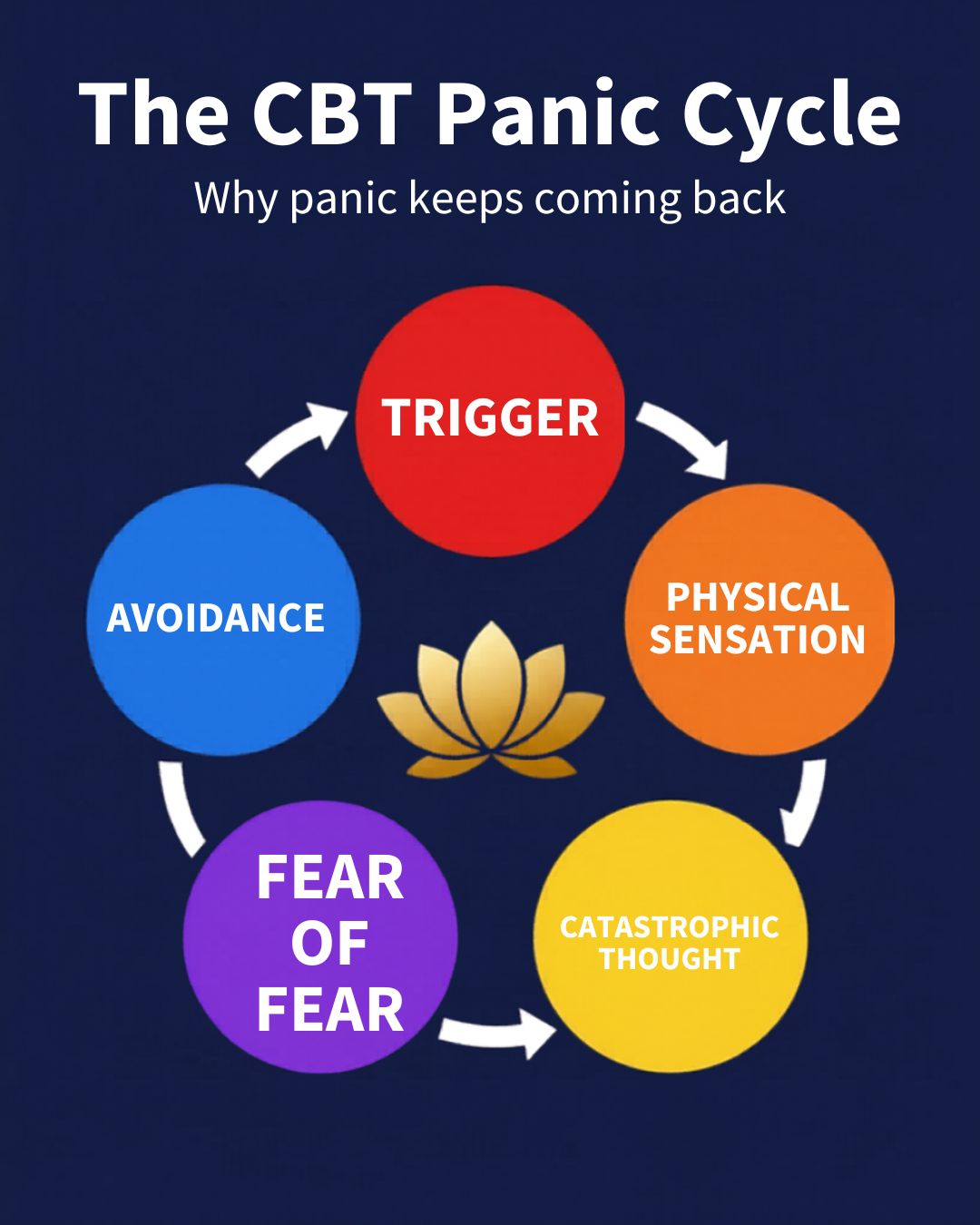
Here’s the painful irony built into that final stage: the avoidance that feels protective is precisely what keeps the cycle running. Every time you avoid a trigger, you send your nervous system the message that the threat was real — and the loop tightens.
Effective therapy for panic disorder doesn’t just reduce symptoms in the moment. It interrupts this cycle at its structural points. Different therapies target different stages — and a skilled panic specialist builds a plan that covers the full loop.
? CBT Insight: Research consistently shows that panic disorder responds exceptionally well to Cognitive Behavioral Therapy — with remission rates of 70–90% in clinical trials. The key is that CBT targets the cognitive and behavioral components of the cycle simultaneously, rather than managing symptoms in isolation.
⚡ Stage 1: The Trigger — What Sets Panic in Motion
Best matched therapy: Cognitive Behavioral Therapy (CBT)
Triggers for panic can be external — a crowded Red Line train, a high-stakes presentation in the Loop, a long drive up Lake Shore Drive — or internal, like a racing heartbeat after too much coffee or a fleeting anxious thought that suddenly snowballs. For many people with panic disorder, the trigger pool expands over time because the nervous system has been trained to stay on persistent high alert.
CBT addresses triggers through a combination of cognitive restructuring and trigger mapping. In early sessions, your therapist works with you to identify exactly what’s activating your threat system — and to examine the automatic interpretations you’re attaching to those triggers before panic even gets underway.
The goal at this stage isn’t to eliminate triggers — that’s neither realistic nor the right aim. The goal is to change your relationship with them: to begin experiencing triggers as activating signals rather than confirmed threats. That cognitive reorientation is where CBT does its most powerful early-stage work for panic.
Our Chicago anxiety therapy services use structured CBT assessment from the very first session to build an accurate trigger map — because knowing what you’re actually responding to is the foundation everything else is built on.
? Stage 2: The Physical Sensation — When Your Body Sounds the Alarm
Best matched therapy: CBT with Interoceptive Exposure
This is the stage that catches most people off guard. In panic disorder specifically, the physical sensations themselves — racing heart, dizziness, shortness of breath, tingling — become triggers in their own right. Your body learns to treat its own normal fluctuations as emergencies. A slightly elevated heart rate after climbing stairs becomes evidence that something is terribly wrong.
A CBT therapist trained in panic disorder will use a technique called interoceptive exposure — deliberately inducing mild versions of the physical sensations you fear in a controlled therapeutic setting. Spinning in a chair to trigger dizziness. Breathing through a narrow straw to mimic breathlessness. Doing jumping jacks to elevate heart rate. It sounds counterintuitive. It’s extraordinarily effective.
The mechanism is clear: when you repeatedly experience the sensation without the catastrophic outcome your brain has been predicting, your nervous system gradually learns that the sensation itself isn’t dangerous. The alarm stops firing quite so loud, quite so fast. See our Chicago CBT Therapy page to learn more.
? Research Note: Interoceptive exposure is one of the most consistently supported components of CBT for panic disorder. Studies show it significantly reduces body-focused anxiety and fear of physical sensations — which are among the most persistent and disabling features of panic disorder. Many clients describe the interoceptive work as the moment treatment finally clicked.
? Stage 3: The Catastrophic Thought — The Story Your Brain Tells
Best matched therapy: CBT + Acceptance and Commitment Therapy (ACT)
This is the cognitive engine of the panic cycle. A physical sensation occurs — your heart skips, your vision blurs momentarily, your chest feels tight — and your brain immediately generates a catastrophic interpretation: “This is a heart attack.” “I’m about to faint in front of everyone.” “I’m losing my mind.”
These thoughts aren’t random. They’re automatic, fast, and deeply reinforced from repetition. And they’re the fuel that transforms an uncomfortable physical sensation into a full-blown panic attack.
CBT tackles catastrophic thoughts directly through cognitive restructuring — identifying the thought, examining the actual evidence for and against it, and building a more accurate interpretation of what’s happening. Over time this process becomes internalized: you catch the catastrophic thought earlier, evaluate it faster, and respond with significantly less panic.
ACT takes a different but complementary angle. Rather than challenging the thought, ACT teaches cognitive defusion — the ability to observe a thought without being swept away by it. Instead of “I’m having a heart attack” becoming your reality, ACT trains you to notice: “I’m having the thought that I’m having a heart attack.” That single cognitive step creates enough distance to interrupt escalation before it takes hold.
Many Chicago CBT therapists integrate both approaches — using CBT’s restructuring in early treatment to build accurate thinking, then layering in ACT’s defusion skills as clients develop greater psychological flexibility.
? Deeper Insight: The catastrophic thought stage is where perfectionism and panic frequently intersect. High-achieving Chicagoans — attorneys in the Loop, executives in the West Loop, medical professionals on the North Side — often report a secondary layer amplifying their panic: “I shouldn’t be feeling this way. I should be able to handle this.” That self-critical overlay is its own trigger. Effective CBT addresses both the panic thought and the perfectionist response to having it.
? Stage 4: Fear of Fear — The Loop That Keeps Panic Going
Best matched therapy: Exposure and Response Prevention (ERP) / Exposure Therapy
This is the stage that separates panic disorder from a one-time panic attack. Fear of fear — clinically called anticipatory anxiety — is when the prospect of having a panic attack becomes its own persistent source of dread. You start scanning your body continuously for early warning signs. You dread situations where panic has struck before. You begin pre-emptively avoiding anything that might trigger the cycle.
The problem: this vigilance is exhausting, and it actually increases the likelihood of panic. A nervous system maintained on constant high alert is a nervous system primed to fire.
Exposure therapy — specifically the structured, graduated approach used in our exposure therapy program — directly targets this stage. Working collaboratively with your therapist, you build a personalized hierarchy of feared situations and systematically approach them, beginning with the least activating and moving methodically up the ladder.
The critical element is what you don’t do during exposure: you resist the safety behaviors — the checking, the reassurance-seeking, the escape planning — that have been keeping the fear alive. Over repeated exposures, your nervous system habituates. The anticipatory dread decreases because the predicted catastrophe keeps not materializing.
For clients whose panic is triggered in specific Chicago situations — driving on Lake Shore Drive, riding the CTA, crowded venues in Wrigleyville — our panic attack toolkit may be particularly helpful.
⚠️ Important: Exposure therapy for panic is not about flooding yourself with fear or “pushing through” at all costs. A well-designed exposure hierarchy is collaborative, carefully paced, and built around your specific triggers and tolerance. If you’ve attempted exposure on your own and found it overwhelming, that’s a signal you need a structured clinical approach — not evidence that exposure doesn’t work for you.
? Stage 5: Avoidance — How Panic Shrinks Your World
Best matched therapy: CBT + ACT + Behavioral Activation
Avoidance is the most visible — and most costly — feature of panic disorder. It starts modestly: skipping the gym because your heart rate spikes. Avoiding the Metra during rush hour. Declining social invitations that feel unpredictable. But over time, avoidance compounds. The world gets smaller. The safe zone shrinks. And the anxiety, paradoxically, intensifies — because every avoided situation confirms to your nervous system that the threat was real and the avoidance was necessary.
CBT addresses avoidance behaviorally — systematically reintroducing avoided situations through the exposure hierarchy while simultaneously restructuring the thoughts driving the withdrawal.
ACT adds a values dimension that many clients find genuinely transformative. Rather than framing treatment as “reducing anxiety,” ACT reframes it as reclaiming your life. The question shifts from “How do I make the panic stop?” to “What would I be doing right now if panic weren’t making the decisions?” That values-based orientation is particularly powerful for clients who’ve been in avoidance mode for years and have lost touch with what they actually want their daily life to look like.
Behavioral Activation — a technique originating in depression treatment but highly applicable to panic-driven avoidance — helps rebuild engagement with meaningful activities in a structured, progressive way. Action creates momentum. Momentum competes with avoidance. And each small approach step begins to renegotiate what your nervous system believes about safety.
Our panic attack therapy program treats avoidance as a primary target, not an afterthought — because for most clients, systematic avoidance reduction is the final barrier between managing panic and actually being free of it.
? When EMDR Belongs in the Picture
Not all panic disorder is purely cognitive and behavioral in origin. For some clients — particularly those whose panic is anchored in a specific traumatic event, a frightening medical episode, a serious car accident, or a history of early adversity — the standard CBT panic cycle tells only part of the story.
When panic attacks are rooted in unprocessed traumatic memory, EMDR (Eye Movement Desensitization and Reprocessing) can be a powerful complement to CBT. EMDR works by reprocessing the stored memory feeding current panic responses — not through repeatedly talking about the trauma, but through a structured bilateral stimulation protocol that reduces the emotional charge still attached to the memory.
A therapist with dual competency in CBT and EMDR can sequence treatment strategically: build stabilization skills through CBT first, then use EMDR to process the underlying material once the client has sufficient internal resources. This integrated approach is particularly effective when panic has a clear traumatic origin point that CBT alone isn’t fully resolving.
? Clinical Note: EMDR is not a first-line treatment for panic disorder without a trauma component. If your panic attacks emerged without a clear traumatic anchor, CBT with interoceptive exposure and structured exposure work is where you want to start. A thorough intake assessment will clarify which approach — or which combination — fits your clinical picture.
? How CBT at the Calm Anxiety Clinic Treats the Full Panic Cycle
At the Calm Anxiety CBT Therapy Clinic in Chicago’s Lakeview neighborhood, we don’t treat panic with a one-size-fits-all protocol. We treat it by mapping your specific cycle — identifying where the loop is tightest, where avoidance has done the most damage, and which stage needs the most direct intervention first.
For most clients, treatment follows a sequenced path:
- Assessment and cycle mapping — building a precise picture of how your panic works, what triggers it, and where avoidance has taken hold
- Psychoeducation — understanding the panic cycle so thoroughly that it begins to lose some of its power; this alone shifts the experience meaningfully
- Cognitive restructuring — targeting the catastrophic thoughts that fuel escalation at Stage 3
- Interoceptive and situational exposure — systematically dismantling the avoidance and fear-of-fear loop at Stages 4 and 5
- Relapse prevention — building the confidence and skills to handle future anxiety without the panic cycle reinstating
For clients who want a more structured, skills-based path through this process, our Pathfinder 10 Program is a 10-session workbook-based treatment that moves through each stage of the cycle with a clear framework and concrete tools. It’s designed for clients who want structure, measurable progress, and a defined endpoint — not open-ended sessions without a clear destination.
We offer in-person sessions at our Lakeview office and telehealth appointments across Illinois — so whether you’re in Andersonville, the West Loop, or downstate, structured panic treatment is within reach.
❓ Frequently Asked Questions About Therapy for Anxiety and Panic
What is the most effective therapy for panic disorder?
Cognitive Behavioral Therapy (CBT) — particularly when it includes interoceptive exposure and structured situational exposure — has the strongest evidence base for panic disorder, with remission rates of 70–90% in clinical trials. For panic with a clear trauma component, EMDR integrated with CBT can be highly effective. The most effective approach is always one tailored to your specific panic cycle, history, and avoidance patterns.
How is therapy for panic disorder different from general anxiety therapy?
Panic disorder treatment is more targeted and more behavioral than general anxiety therapy. It addresses the panic cycle directly — the physical sensations, the catastrophic interpretations, the fear of fear, and the avoidance — rather than working primarily on worry and rumination. Interoceptive exposure, which deliberately induces mild physical sensations to reduce fear of them, is specific to panic treatment and not typically part of general anxiety work.
How long does therapy for panic disorder take?
Many clients see significant improvement within 12–20 sessions of structured CBT for panic disorder. The Pathfinder 10 Program at the Calm Anxiety Clinic delivers a complete treatment framework in 10 structured sessions. More complex presentations — with significant avoidance, comorbid depression, or a trauma component — may benefit from a longer treatment course.
Can panic disorder be treated without medication?
Yes. CBT is an effective standalone treatment for panic disorder and is often preferred by clients who want to address the root cycle rather than manage symptoms pharmacologically. Some clients benefit from a short course of medication to reduce panic frequency enough to fully engage with the CBT work — particularly when attacks are occurring multiple times per week. A discussion with your therapist and, where relevant, a prescriber will clarify the right approach for your situation.
What’s the difference between anxiety and panic disorder?
Anxiety is characterized by persistent worry, dread, and tension — typically future-focused and more diffuse. Panic disorder involves discrete, intense episodes (panic attacks) with pronounced physical symptoms, followed by persistent fear of future attacks and significant avoidance behavior. Many people experience both simultaneously. Our post on the difference between stress, anxiety, and depression covers this distinction in depth.
Does exposure therapy for panic work if you’ve struggled for years?
Yes — the duration of panic disorder doesn’t significantly predict treatment outcome in CBT. What matters more is the quality and structure of the exposure work and the degree to which avoidance is systematically addressed. Many clients who’ve managed panic disorder for a decade or more achieve full remission with a well-designed CBT treatment plan.
What if I’ve tried CBT before and it didn’t help?
This is worth exploring carefully with a new therapist. CBT for panic disorder is a specific protocol — not all CBT is equivalent, and therapy delivered without interoceptive exposure, structured hierarchies, or direct work on avoidance is unlikely to produce the results the research promises. If previous CBT felt like generic talk therapy with occasional thought records, you likely haven’t experienced the full panic-focused protocol. A consultation with a specialist is worth pursuing before ruling it out.
How do I find a panic disorder specialist in Chicago?
Look for a therapist with specific training in CBT for panic disorder and demonstrated experience with interoceptive exposure and ERP techniques. General talk therapy or supportive counseling, while valuable for many concerns, typically doesn’t address the panic cycle with the precision panic disorder requires. The Calm Anxiety CBT Therapy Clinic specializes in panic attack therapy in Chicago, with in-person sessions in Lakeview and telehealth available across Illinois.